
Stroke Examination Tools
 Early recognition and prompt medical evaluation is critical for the use of thrombolytic therapy for patients with acute ischemic stroke9. Early detection of stroke is essential in order to improve outcomes and decrease long-term disability. Clinicians in both out-of-hospital settings and in-hospital settings use various tools to determine the likelihood of stroke in patients with symptoms suggestive of stroke.
Early recognition and prompt medical evaluation is critical for the use of thrombolytic therapy for patients with acute ischemic stroke9. Early detection of stroke is essential in order to improve outcomes and decrease long-term disability. Clinicians in both out-of-hospital settings and in-hospital settings use various tools to determine the likelihood of stroke in patients with symptoms suggestive of stroke.
Quick recognition in the prehospital setting allows the receiving facility to mobilize the stroke team as the patient is being transported to the facility. To accomplish this, clinical centers have emphasized “prehospital education” and “en-route notification by EMS personnel.”1 Notifying the emergency department that the patient is likely suffering a stroke can lead to quicker imaging, which in turn means faster delivery of fibrinolytic therapy or PCI (percutaneous coronary intervention).
Acute stroke treatment is time-dependent, and the faster a stroke can be identified, the better the outcome for most patients. The expression “time is brain” has become the mantra of acute stroke treatment, as an estimated 1.9 million neurons are lost each minute that a stroke is left untreated, and patient outcomes are substantially improved with shorter treatment times.4 As a response to the need for standardized stroke assessment, various stroke screening tools or scales have been developed. Although the scales do not predict the outcome after a stroke, they can be very useful as a triage tool. A standardized scale also helps prevent variations among emergency service personnel and first responders who are evaluating a patient for stroke.
Scales in Use
There are multiple scales that are commonly used worldwide in the assessment of stroke victims, including the five listed below:
- National Institutes of Health Stroke Scale (NIHSS)
- Cincinnati Prehospital Stroke Scale (CPSS)
- Face Arm Speech Test (FAST)
- Los Angeles Prehospital Stroke Screen (LAPSS), and
- Recognition of Stroke in The Emergency Room (ROSIER)
The National Institutes of Health Stroke Scale (NIHSS)
The National Institutes of Health Stroke Scale (NIHSS) was designed as a research tool to measure stroke severity.2 The NIHSS has evolved beyond academic research and has become the gold standard for clinical stroke assessment and measurement.6 The NIHSS is a valuable tool for both initial assessments of stroke severity and ongoing assessment to monitor for actionable changes in patient condition.3
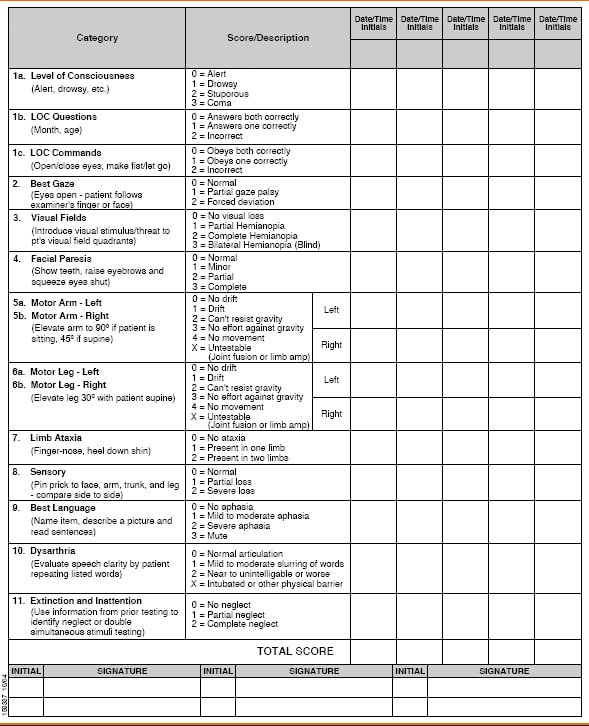
This stroke scale may be used to identify the likelihood of a stroke, and can also estimate severity. It measures 15 clinical functions or deficits such as gaze, vision, level of consciousness and facial palsy. Limb ataxia, sensory loss, dysarthria and language are also measured. Arm and leg strength, along with inattention, are also evaluated. The items must be administered in order and without patient coaching. Although it may be completed in six to ten minutes, the assessment is far longer than some other stroke scales.
The Cincinnati Prehospital Stroke Scale (CPSS)
The Cincinnati Prehospital Stroke Scale (CPSS) was derived from a simplification of the 15-item National Institutes of Health Stroke Scale (NIHSS) and evaluates the presence or absence of facial palsy, asymmetric arm weakness, and speech abnormalities in potential stroke patients5. This scale tests for three possible signs of stroke, including facial droop, arm drift and speech abnormality. One abnormal finding out of three means that there is a greater than 70% chance that the patient is experiencing a stroke, while three abnormal findings indicate a >85% probability of stroke.
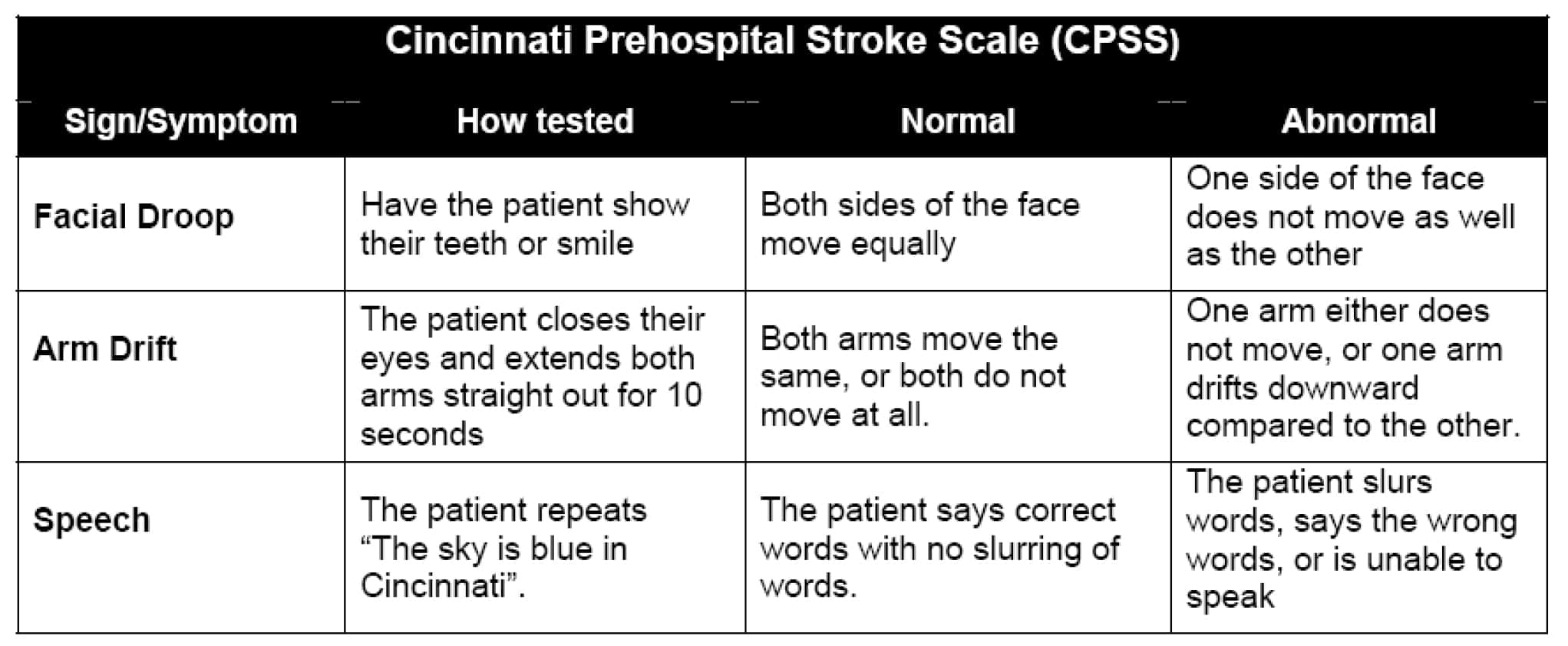
An obvious advantage of using the Cincinnati Prehospital Stroke Scale is that it is fast. The evaluation can usually be completed in less than a minute. In some situations, using the fastest stroke scale may be most beneficial. One possible disadvantage to using this stroke scale is that it only based on a few parameters, and therefore may not be an efficient way to assess for a posterior circulation stroke, which may cause symptoms such as dizziness and vomiting and is responsible for 5 to 10% of all ischemic strokes.
Face Arm Speech Test (FAST)
The FAST was developed in 1998 as a stroke identification instrument by a group of stroke physicians, ambulance personnel, and an emergency room physician, and was designed to be an integral part of a training package for UK ambulance staff.5
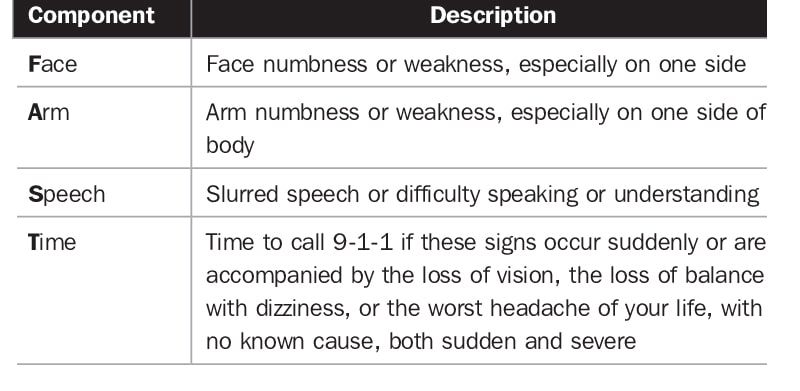
The FAST contains three key elements (facial weakness, arm weakness, and speech disturbance) but avoids the need to repeat a sentence as a measure of speech, instead using assessment of language ability by the paramedic during normal conversation with the patient.5
The Los Angeles Prehospital Stroke Screen
The LAPSS is a longer instrument consisting of four history items, a blood glucose measurement, and three examination items designed to detect unilateral motor weakness (facial droop, handgrip, and arm strength).5 The scale takes into consideration the patient’s age, whether or not the patient has ever had a seizure, the length of time symptoms have been present, and whether at baseline the patient is bedridden or wheelchair-bound.
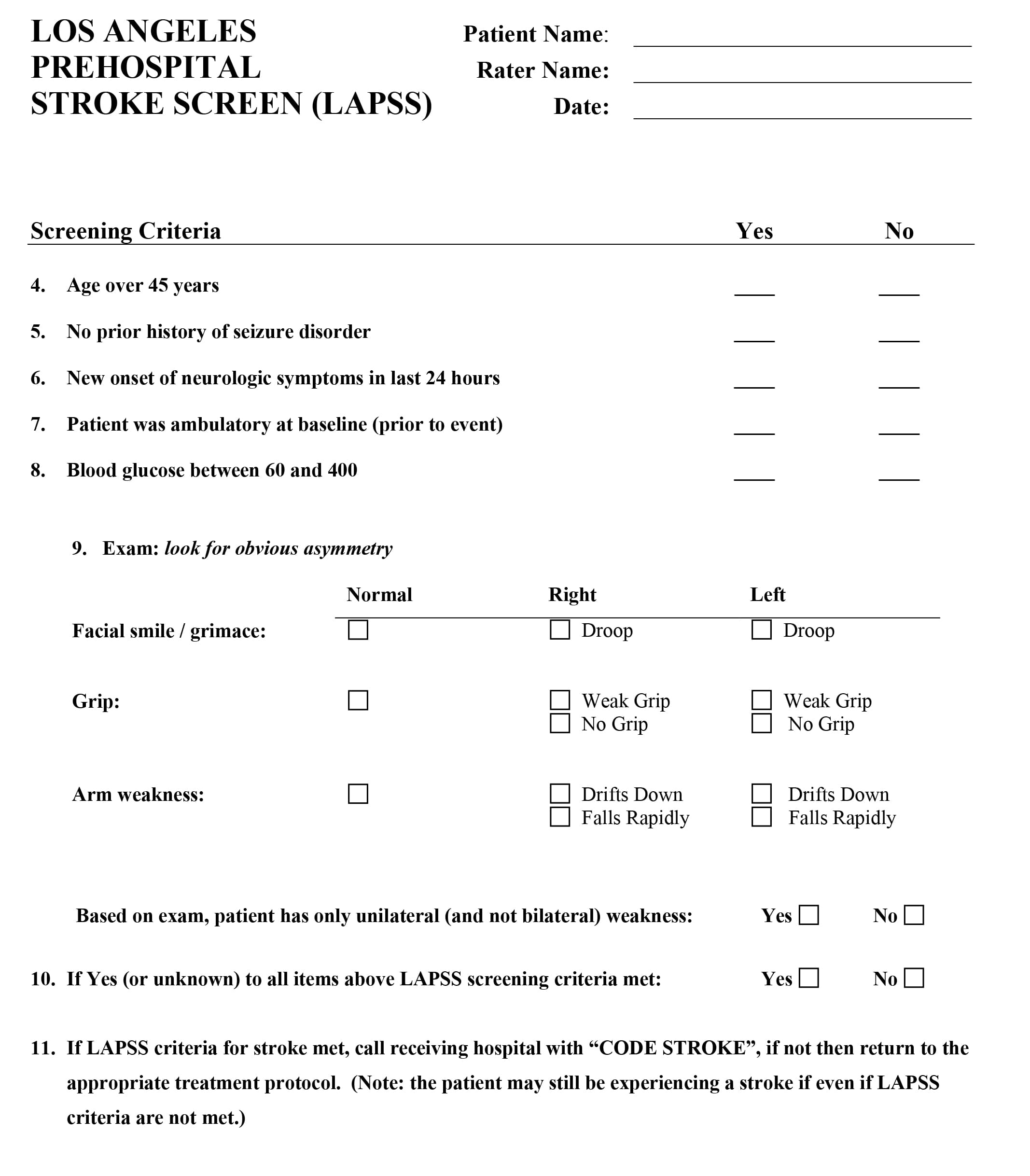
The main drawback to using the Los Angeles Prehospital Stroke Screen is that it may take slightly longer to complete than the more succinct Cincinnati Prehospital Stroke Scale.
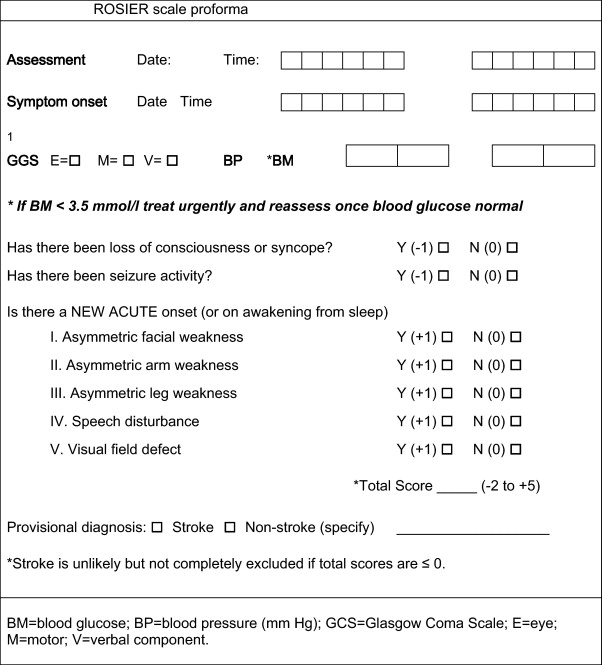
Recognition of Stroke in the Emergency Room (ROSIER)
The ROSIER assesses elements of history and physical examination to produce a score between 2 and 5. Patients with a total score of >0 are taken as being consistent with stroke, whereas scores of 0 signify a low probability of stroke.10
One benefit of using a stroke scale is that it provides a standardized tool for initial neurological evaluation. The type of scale selected may vary depending on employer or facility policy. For example, certain emergency service agencies may utilize a specific stroke scale. If personnel have the option to use different stroke scales, they should choose a scale that appears to be appropriate for the situation and the patient’s condition. They should also use a scale with which they are very familiar.
It is difficult to say which scale is superior to another. Different situations may call for the use of different scales. For example, if a rapid assessment needs to be performed, the Cincinnati Prehospital Stroke Scale may be the most advantageous. In other situations, a more thorough assessment may be warranted. It is also important to keep in mind that, although a stroke scale is a useful tool, it is only one piece of the puzzle.
References
- Barsan WG, Brott TG, Broderick JP, et al: Time of hospital presentation in patients with acute stroke. Archives of Internal Medicine. 1993;153:2558-2561.
- Brott T, Adams HP Jr, Olinger CP, et al. Measurements of acute cerebral infarction: A clinical examination scale. Stroke. 1989;20(7):864-870.
- Dancer S, Brown AJ, Yanase LR. National Institutes of Health stroke scale in plain English is reliable for novice nurse users with minimal training. Journal of Emergency Nursing. 2017;43:221-227.
- Fonarow GC, Zhao X, Smith EE, et al. Door-to-needle times for tissue plasminogen activator administration and clinical outcomes in acute ischemic stroke before and after a quality improvement initiative. JAMA. 2014;311:1632-1640.
- Harbison K, Hossain O, Jenkinson D, Davis J, Louw SJ, Ford GA. Diagnostic accuracy of stroke referrals from primary care, emergency room physicians, and ambulance staff using the face arm speech test. Stroke. 2003;34:71-76.
- Hinkle JL. Reliability and validity of the National Institutes of Health stroke scale for neuroscience nurses. Stroke. 2014;45(3):e32-e34.
- Juach E, Cucchiara B. 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010. http://circ.ahajournals.org/content/122/18_suppl_3/S818.full. Accessed August 2014.
- Kidwell CS, Startman S. Identifying stroke in the field; Prospective validation of the Los Angeles prehospital stroke screen. http://www.ncbi.nlm.nih.gov/pubmed/10625718. August 2014.
- Kothari RU, Panciolo A, Liu T, Brott T, Broderick J. Cincinnati prehospital stroke scale: Reproducibility and validity. Annals of Emergency Medicine. 1999;33:373-378.
- Mingfeng H, Zhixin W, Qihong G, Lianda L, Yanbin Y, Jinfang F. Validation of the use of the ROSIER scale in prehospital assessment of stroke. Annals of the Indian Academy of Neurology. 2012;15:191-5.

