
Breaking Down Patient Assessment: Deconstructing the Primary Survey
 During my time in EMS, I have had the privilege to work with some amazing EMTs and paramedics, men and women who exemplify professionalism in healthcare and inspire others to push themselves farther in both their education and clinical care. We all know the type: intuitive, compassionate, and always up to date on the latest medical knowledge. In my early years, I was partnered with such a paragon of medical care, a medic who I will call Diana. She had been my preceptor when I was first hired as an EMT at our local, small county-run EMS service and was widely considered one of the smartest providers on staff. One particular memory of our time together had to do with a respiratory patient we ran one evening. As we walked in, we noted an elderly female sitting upright in her chair. Diana looked the patient up and down, put her hand on the patient’s chest, and then told me that we needed the CPAP and the stretcher. At the time, I had no idea how she was able to determine so quickly what was wrong with our patient. As years have gone by, I have come to understand the “secret,” such as it is.
During my time in EMS, I have had the privilege to work with some amazing EMTs and paramedics, men and women who exemplify professionalism in healthcare and inspire others to push themselves farther in both their education and clinical care. We all know the type: intuitive, compassionate, and always up to date on the latest medical knowledge. In my early years, I was partnered with such a paragon of medical care, a medic who I will call Diana. She had been my preceptor when I was first hired as an EMT at our local, small county-run EMS service and was widely considered one of the smartest providers on staff. One particular memory of our time together had to do with a respiratory patient we ran one evening. As we walked in, we noted an elderly female sitting upright in her chair. Diana looked the patient up and down, put her hand on the patient’s chest, and then told me that we needed the CPAP and the stretcher. At the time, I had no idea how she was able to determine so quickly what was wrong with our patient. As years have gone by, I have come to understand the “secret,” such as it is.
Diana had a knack for making incredibly accurate field diagnoses, something that many medics at the time shied away from. In those days, the common philosophy was that it was not our job to diagnose anything. We were just responsible for keeping the patient alive long enough to get them to definitive care in the ER. Diana felt differently, often saying, “How can I be expected to treat a patient appropriately if I can’t make a field diagnosis?” As I have gotten older, I have come to believe the same. Furthermore, I firmly believe that our ability to form an accurate field diagnosis lies mainly with the clinician’s ability to perform a thorough primary assessment. To that end, let us look at the different components of the primary assessment in an effort to better understand how to more effectively utilize it.
The primary assessment (or primary survey, depending on your chosen vernacular) is meant to do one thing and one thing only: detect and correct immediate or imminent life threats. The long-standing process has been to assess the patient’s mental status as well as their ABCs, fixing the aforementioned threats as they are found. But what exactly are the criteria of a “life threat?” Most first-year EMT and paramedic students will shout out in almost perfect unison, “Anything that threatens the patient’s respiratory or cardiovascular status!” Of course, they would not be wrong in a general sense. However, medicine is never that simple.
There are many disease processes that can affect the integrity of the patient’s airway, but depending on when the clinician encounters the patient, the said disease process may or may not be a discernible life threat. That is why there is a caveat that must be added to our “threat” criteria. To be truly honest, in all reality, you can get rid of everything BUT the caveat. To make it simple, we can say that a life threat occurs when something interrupts the ability of your patient to maintain perfusion, whether systemically or locally. For example, a patient could present with the signs and symptoms of an early asthma attack. You may note light wheezing and a slightly increased work of breathing. However, his airway is patent, his breathing is adequate, and his circulation is uncompromised. This patient is not experiencing an immediate life threat. But let us look at the same patient a few hours later, assuming he received no care. The patient now presents with significant wheezing, heavy work of breathing, altered mentation, tachypnea, tachycardia, and appears cyanotic around his lips and conjunctiva. This patient is experiencing an interruption in his ability to maintain perfusion, and is experiencing a life threat. With that in mind, as we break down the primary assessment, let’s remember that all in all, we are assessing the ability of the patient to perfuse adequately.
The General Impression
The primary assessment will usually always begin with the general impression (GI). While some struggle to identify what this entails, at its core the general impression is nothing more than what you see when you first set eyes on your patient. Essentially, we are determining if our patient is “sick (not stable)” or “not sick (stable),” thus deciding whether the patient will likely need emergent or non-emergent interventions. This ability improves as we gain more experience through patient encounters, resulting in an increased likelihood of identifying patients who are sick vs those who are not sick. This determination is based on multiple factors, most of them on the opinion of the clinician. But though the GI is subjective in nature, with an experienced practitioner it can be very accurate.
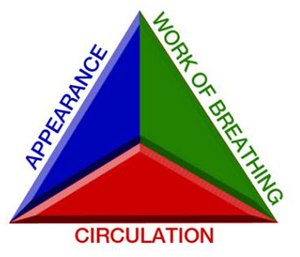 While we eventually expect providers to make this sick/not sick determination fairly quickly, we also know that this is a skill that takes time. To help newer clinicians, we suggest utilizing the Patient Assessment Triangle in their decision-making algorithm. The three sides of the triangle represent the three components of the GI: patient response (appearance), work of breathing, and skin presentation (circulation). If the patient responds well to the provider during their introduction, or at least tracks their movement around the room, then we would mark that as a “positive” appearance score. If this same patient were sitting in the tripod position with labored breathing and pale skin, we would say they had a “negative” work of breathing and circulation score and thus, is sick. Likewise, if the patient appears somnolent but does not have an increased work of breathing and pink/warm skin, they are still sick. It only takes one leg receiving a negative score for the PAT to be considered abnormal. Of course, due to the subjective nature of the GI, patients who are initially deemed “sick” may in fact be stable, while those who are thought to be “not sick” can certainly later be found to be unstable. This will be better determined later in the primary assessment.
While we eventually expect providers to make this sick/not sick determination fairly quickly, we also know that this is a skill that takes time. To help newer clinicians, we suggest utilizing the Patient Assessment Triangle in their decision-making algorithm. The three sides of the triangle represent the three components of the GI: patient response (appearance), work of breathing, and skin presentation (circulation). If the patient responds well to the provider during their introduction, or at least tracks their movement around the room, then we would mark that as a “positive” appearance score. If this same patient were sitting in the tripod position with labored breathing and pale skin, we would say they had a “negative” work of breathing and circulation score and thus, is sick. Likewise, if the patient appears somnolent but does not have an increased work of breathing and pink/warm skin, they are still sick. It only takes one leg receiving a negative score for the PAT to be considered abnormal. Of course, due to the subjective nature of the GI, patients who are initially deemed “sick” may in fact be stable, while those who are thought to be “not sick” can certainly later be found to be unstable. This will be better determined later in the primary assessment.
Level of Consciousness
The second step in the primary assessment is to establish the patient’s level of consciousness. Here, the provider is attempting to determine if the patient is alert to time/place/event or if they are displaying any deficits of awareness. This is evaluated by using the AVPU (alert, verbal response, pain response, or unresponsive) mnemonic. If, after the EMT or paramedic introduces themselves, the patient responds appropriately, then they would be considered alert. If the clinician noted that the patient’s eyes were closed, or they exhibited a blank stare, only verbally responding when their name is called, then they would be considered responsive to verbal stimuli. If the patient only responds to some sort of physical stimuli, such as a sternal rub or trapezius pinch, then we would say they are responsive to pain. Lastly, if the patient has responded to none of the above, we would say they are unresponsive.
Now, a note on painful stimuli. There have been a few cases where the utilization of painful stimuli to elicit a response has been viewed as assault. Providers, in the heat of the moment, may too vigorously perform a sternal rub, bruising the sternum. Remember, the term painful does not actually denote the use of pain but instead references the use of external stimulus in efforts to get the patient to respond to their external environment. A light pinch or chest rub will typically suffice. Additionally, remember that the presence of a gag reflex would technically indicate a painful response, as the patient is reacting to an outside stimulus.
The Glasgow Coma Scale was originally developed to assess and document the severity of brain dysfunction, with descriptions that medical professionals at all levels of training could understand, even if English was not their primary language. The categories assessed when evaluating a patient are eye opening, motor response, and verbal response, each category receiving a certain number of points with a maximum score of 15. Today, providers use the Glasgow Coma Score to assess patient survivability. Patients with scores between 13 and 15 are considered mildly impaired and will often fully recover. Patients with scores between 9 and 12 are categorized as moderately disabled. Patients with GCS scores of 3 to 8 are often comatose, unconscious with no purposeful movements, have no interaction with their environment, or have no localized response to pain. Approximately 50% of patients with a score of 8 will be unconscious or in a coma, and almost all patients with a score of 7 or less will be unconscious or in a coma. A patient with a GCS of 3 is either dead or in a vegetative state with possible sleep-wake cycles (Sippel 2011). Additional modifications to the Glasgow Coma Scale include response levels for small children. While most patients will not receive a GCS during their assessment, multi-system trauma patients are almost certainly going to require one prior to being deposited at the local trauma center.
Airway, Breathing, and Circulation
We now come to the portion of the primary assessment where a more objective approach is required. Keeping in mind that this assessment is looking to determine the adequacy of systemic perfusion, we must ask ourselves the following: is the patient ventilating? Is the patient oxygenating? Is the patient respirating?
To answer these, we must first define what those terms mean.
- Ventilation refers to the mechanical aspect of breathing. The chemoreceptors in the brain signal that there is too much carbon dioxide in the body. This causes a chain reaction where the diaphragm drops down, expanding the intrathoracic cavity. Oxygen-rich air flows into the lungs and down to the alveoli, where diffusion will take place. Once the oxygen and carbon dioxide have swapped places, the Hering-Breuer reflex will be triggered, signaling the body to exhale, resulting in the relaxation of the diaphragm and the expelling of carbon dioxide.
- Oxygenation refers to the external loading of oxygen into the cardiopulmonary system, essentially the movement of oxygen from the outside environment to the cells within tissues, and the transport of carbon dioxide in the opposite direction. During oxygenation, diffusion takes place, replacing carbon dioxide from oxygen-depleted blood with oxygen from the alveoli.
- Respiration occurs when oxygen molecules are dispersed systemically throughout the body, entering the cells to make ATP.
When all 3 of these anatomic and physiologic processes work together, perfusion occurs (Jeff 2019).
Airway
Assessment of the airway evaluates the patient’s ability to ventilate, though not necessarily that they ARE ventilating. The first question the provider must ask themselves is: if the patient WAS able to breathe, COULD they breathe? This refers to airway patency. If the airway is open, then you can move forward. If not, then we must open the airway, either via the “head-tilt, chin-lift” or “jaw-thrust” maneuvers. If the patient has secretions in their airway, then they will need to be suctioned. If the patient is not able to maintain airway patency on their own, then an airway adjunct must be placed.
Breathing
Assessment of the patient’s breathing confirms their ability to ventilate and assesses the ability to oxygenate. The provider must first assess the rate, rhythm, and quality of the patient’s respirations. An increased or decreased rate, irregular respiratory pattern, or decreased quality of breathing could all result in inadequate respiration. The clinician should then auscultate the patient’s breath sounds, noting anything abnormal such as wheezing, rales, or rhonchi. Lastly, the provider must determine if the patient requires some form of oxygen. If the patient is able to maintain their own airway and has adequate respirations, then a nasal cannula or non-rebreather mask will generally suffice. However, if this is not the case, then artificial ventilation will be required via bag-valve-mask. If you are on the fence as to whether the patient needs oxygen or not, then continue forward with your assessment.
Circulation
Assessment of the patient’s circulation will confirm their ability to perform internal respiration. The provider begins by assessing the rate, rhythm, and quality of the patient’s pulse, much for the same reason as with their breathing. Any bleeding that has not already been controlled or noted, but presents as a direct life threat, should be dealt with at this time. Lastly, the skin should be thoroughly assessed as it is one of the most reliable diagnostic tools when determining systemic perfusion. If the patient is not respirating efficiently, this will be reflected in their skin color and condition. The presence of cyanosis, pallor, or mottling all are indicative of poor perfusion.
Disposition and Transport
The disposition and transport of patients depends on multiple factors, both objective and subjective. Many times, it may be nothing more than a gut feeling that results in the mode in which the patient is transported to the emergency room. In the end, the provider must take into account all of the factors presented in the primary assessment in order to make the most appropriate decision for the patient.
The Absence of Technological Diagnostics
One factor that is noticeably absent from our breakdown of the primary assessment is the use of technological diagnostic tools. While the provider will obtain manual pulse and respiratory rates, no other tools are utilized or even needed during this assessment. This can make some clinicians uncomfortable, particularly those who are newer to the profession. But there are some very good reasons why the pulse oximeter and the blood pressure cuff are left behind when completing the primary assessment, all of which boil down to this: time is a factor and you don’t need those tools to determine a life threat.
Let’s consider the blood pressure cuff, which certainly has its uses, particularly during the secondary assessment. Other than what the patient’s actual blood pressure is, what are you going to gain from this knowledge that will impact your initial care of the patient? You don’t need to know if your patient’s blood pressure is higher or lower than normal. All you need to be concerned about at this time is whether you have a high enough systolic pressure to support peripheral perfusion. We know that in a vast majority of adults this equates to a systolic of 90mmHg (Deakin 2000). Moreover, we know that most adults must have this same systolic pressure in order to have a radial pulse. Therefore, when assessing for a radial pulse during the “circulation” portion of the ABCs, we can easily determine whether the patient currently has a pressure high enough to support peripheral perfusion.
As we covered under “circulation,” skin is a much more reliable diagnostic tool than anything you have in your bag. Assessing the patient’s skin color, temperature, and condition can provide a monumental amount of knowledge. Abnormal skin color may include pallor, cyanosis, flushing or redness, mottling or jaundice. Cyanosis is a late sign of hypoxia or poor perfusion states. Redness or flushing is typically a result of peripheral vasodilation. Pallor is an early sign of hypoxia and is also seen in poor perfusion states. Mottling occurs when blood stagnates in an area of poor perfusion and becomes deoxygenated. Jaundice, a yellow coloring of the skin and sclera, is a sign of hepatic failure. Abnormal skin temperatures may be cool, cold, or hot. When assessing the skin, be sure to take into account the ambient temperature. Hot skin temperature may be an indication of a significantly increased body core temperature. Peripheral vasoconstriction will cause the warm red blood in the skin to be shunted to the core of the body, resulting in cool skin temperature. Cold skin usually occurs as a result of a significant decrease in the body’s core temperature. Capillary refill is a useful test of hydration status in pediatric patients. The best place to test for capillary refill in children is on the forearm or over the patella.
Conclusion
Hopefully, this breakdown of the primary assessment has been useful not just to newer providers but to more seasoned practitioners as well. When looking at the entire article in written form, one would think that this process would take anywhere from 15-20 minutes just to complete. However, those who work in the profession know that the primary assessment shouldn’t take much longer than a few minutes to complete, regardless of how sick the patient is. In part II, I will address the secondary assessment and its comprehensive nature. Remember, patient assessment is not a skill we learn in class and then forget once we are in the field. Skilled providers spend years perfecting their patient assessment techniques, only to find new information and ways to treat their patients. Always be open to possibilities as medicine will always be a practice, not a certainty.
Check Your Knowledge
- What are the differences between ventilation, respiration, and oxygenation?
- What are some key indicators of adequate perfusion?
- Why is it NOT necessary to use tools such as pulse oximeters and blood pressure cuffs during the primary assessment?
References
- Deakin CD, Low JL. Accuracy of the advanced trauma life support guidelines for predicting systolic blood pressure using carotid, femoral, and radial pulses: observational study. BMJ. 2000;321:673–674.
- Understanding ventilation vs. oxygenation is key in airway management. JEMS. November 19, 2012. Accessed Oct 7, 2020. https://www.jems.com/2012/11/19/understanding-ventilation-vs-oxygenation/.
- Sippel R. EMS Recap: The Glasgow Coma Scale. June 23, 2011. Accessed Oct 7, 2020. https://www.emsworld.com/article/10318723/ems-recap-glasgow-coma-scale.
 Andrew R. Ross—MHA, NRP—has worked in the EMS industry as a paramedic for 19 years. He is a lead educator at Careercert and has over a decade of experience in EMS education and management. Andrew currently works full-time as the lead faculty instructor in his local community college’s EMS program. As an education advocate, Andrew recently earned his master’s in healthcare administration from the University of Scranton. He is married and has 2 daughters.
Andrew R. Ross—MHA, NRP—has worked in the EMS industry as a paramedic for 19 years. He is a lead educator at Careercert and has over a decade of experience in EMS education and management. Andrew currently works full-time as the lead faculty instructor in his local community college’s EMS program. As an education advocate, Andrew recently earned his master’s in healthcare administration from the University of Scranton. He is married and has 2 daughters.


